What is obstructive sleep apnea? In short terms, it’s a disorder that causes breathing to stop and start while you’re sleeping. Sounds scary, right? I mean, it really is. There are several different types of apnea, but this one is the most common. It is said to affect approximately 4% of men and 2% of women, but only around 10% actually seek treatment while the others go undiagnosed.

This is a relatively common sleep disorder, affecting around 20 million Americans. The scary part about this disease is that it often goes unrecognized, meaning a person who has it doesn’t actually know that they are suffering from something that can cause future problems with their health. Without snoring, it’s very difficult to even realize that you have obstructive sleep apnea.
Obstructive Sleep Apnea Causes
This is one of those disorders that do have a cause for the issue. The cause of obstructive sleep apnea syndrome is while you’re sleeping, the muscles that are responsible for controlling the throat and tongue relax. When this happens, either you snore or your airway could completely collapse, causing your breathing to come to a halt. The tissue in the back of your throat can also sag, which narrows and constricts the airway.

OSA is generally characterized by episodes of shallow or paused breathing and it happens repetitively. These episodes usually come with a reduction of blood oxygen saturation. Those who suffer from this are usually unaware until they are diagnosed or their spouse or friend recognize the issues that are happening.
There are quite a few other causes that you wouldn’t generally think of, but they are directly related to the relaxation of the muscles and irritation.
— Smoking

Smoke inhalation irritates the throat, lungs, and esophagus. This can also irritate the throat muscles, causing them to relax to the point of blocking your airway while you’re sleeping.
— Natural Causes

There are those who are just naturally predisposed to having a more narrow throat or an enlarged tongue. If you have a family history of OSA, you are more probable to have it yourself.
— Age

The older people get, the more they lose muscle tone. As the throat muscles lose their definition, they will become more weak and are more likely to collapse and block your airway while sleeping.
— Enlarged Tonsils or Adenoids
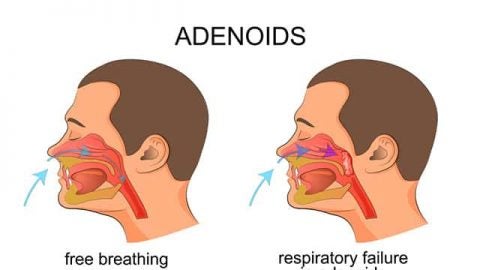 This is the leading cause of OSA in children and babies, but it can also have an effect on adults who never had a tonsillectomy as a child or teen.
This is the leading cause of OSA in children and babies, but it can also have an effect on adults who never had a tonsillectomy as a child or teen.
— Diabetes

Obstructive sleep apnea studies have shown that this condition may be more common in those who suffer from diabetes.
— Asthma
 Research performed recently has shown that there is an association between the risk of OSA and asthma.
Research performed recently has shown that there is an association between the risk of OSA and asthma.
— Gender
 Males are twice more likely to suffer from the condition than women are.
Males are twice more likely to suffer from the condition than women are.
— Pregnancy

Hormones that come with the miracle of pregnancy can congest the mucous membranes of the upper airway, which increases the odds for sleep apnea.
— Weight

It has been shown that in most cases, a person’s weight has a direct link to OSA. People who are more overweight than others are more likely to have some form of apnea than those who are healthier in weight. The reason for this is because the excess fatty tissues become built up in the neck and throat, leading to airflow restrictions.
You may interested in: Sleep and Obesity: The Link Between Sleep And Weight
Complications
OSA is a recognized cause for secondary hypertension. During the night, the systolic and diastolic pressure that keep blood pressure elevated at night have surges caused by the sleep apnea. It’s important that you get screened for OSA if you suffer from hypertension because the longer you have these surges, the higher your cardiovascular risk becomes.

If you have OSA, you can also suffer from complications with medications and surgery. Medications, such as sedatives, narcotic analgesics, and general anesthetics can relax your upper airway even more, worsening your OSA.

Eye problems are another complication of apnea. Some research has found that there’s a link between certain eye conditions and sleep apnea such as glaucoma. Luckily, they can usually be treated.

One other complication that can come from this condition is a sleep-deprived partner. If you don’t have one, then you don’t have to worry about this, but if you do, keep reading. Loud snoring can keep those who are near you from getting any sleep. This can even have an effect on your relationship. If your partner has a concern and you don’t yet have a diagnosis, go get checked.
Symptoms
Sometimes, those with OSA can’t recognize their own symptoms. One of the main giveaway’s of the disorder is snoring. This happens when the airway is restricted, causing vibrations. During an apnea event, your air is restricted, which restricts the flow of blood to the brain. This signals the brain to awaken the part of the way to tell the body it needs to breathe. This is usually followed by a loud gasping sound. It could also sound like choking or snorting. Once the suffering person breathes, the brain goes back to sleep and the process can happen over and over again.

Those who suffer from mild OSA will have an episode 5-14 times per hour, moderate OSA sufferers will have 15-30 per hour and those with severe OSA will experience more than 30 interruptions in sleep per hour.
Here is a simplified list of what the symptoms associated with OSA are:
- Restless sleep
- Snoring
- Depression
- Irritability
- Headaches in the morning
- Daytime fatigue
- Frequent breathing breaks
Treatment For OSA
The treatment for obstructive sleep apnea can vary depending on how severe the condition is. There are actually eight main treatments that are available and you may qualify for a home sleep test or assessment to determine how severe your condition is. These are issued to patients who are more likely to have apnea and need their severity determined. Depending on what the tests show, there are multiple therapy options available.
#1. Positive Airway Pressure Therapy
— CPAP or Continuous Positive Airway Pressure Machine
One of the most common therapies for PAP is a CPAP or continuous positive airway pressure machine. These devices are most commonly used for patients with OSA. The CPAP works by allowing air to be gently pressurized through your airway, keeping your throat from collapsing. These machines are generally easy to use and consist of the monitor, hoses and a mask. You need to use the machine regularly to help alleviate your condition. This is not a cure. It is simply a therapy.
— APAP or Automatic Positive Airway Pressure Machine
Another therapy device is an APAP. This stands for automatic positive airway pressure and uses the same basic principles as the CPAP machine. However, the APAP is more complex when it comes to the pressure setting. This machine uses algorithms that can sense changes in your breathing and it will then adjust the settings at any time throughout the night. This is not a cure. It is simply a therapy.
You may want to read: BiPAP VS CPAP Machine
— BiPAP or Bilevel Positive Airway Pressure Machine
The more advanced treatment in this category would be the BiPAP. This stands for bilevel positive airway pressure. This machine has the ability to include a breath timer that measures how many breaths are taken per minute. If your breathing exceeds the limit, the machine can force the person to breathe by temporarily increasing the air pressure.
#2. Oral Appliance Therapy
One of the most common oral appliances to help fight against sleep apnea is a mandibular advancement device. This is a device that fits in the mouth and moves the jaw forward. This helps eliminate any restriction that can happen in the back of the throat by moving the jaw away from the back of your throat, thus increasing the upper airway size.
Another oral appliance is a tongue retaining device. This piece of equipment simply holds the tongue forward while you’re sleeping, preventing obstruction of the airway.
You may want to read: Mouth Guards for Sleep Apnea
#3. Surgery

If it comes down to it, there are several surgical options available such as a uvulopalatopharyngoplasty, adenotonsillectomy, nasal surgery and maxillomandibular advancement. These are usually last resorts if other treatments do not work because of how invasive they are.
#4. Exercises
Of course, there are exercises that come with sleep apnea! This may be something that the doctor will ask you to do before anything else or it may be along with your device.
- Do 20 reps of pushing the tip of your tongue against the roof of your mouth while sliding it backward.
- Do 20 reps of sucking your tongue upward so that it’s completely against the roof of your mouth.
- Force the back of your tongue down against the bottom of your mouth while keeping the tip of it in contact with your bottom front teeth.
You may want to read: Know About Mouth Guards for Sleeping
Conclusion
Obstructive sleep apnea can be a scary condition, especially if you don’t know that you have it. Luckily, there are more than one option to treat it and some warning signs that can point you in the direction of your healthcare provider. If you snore or your partner tells you that you seem like you’re gasping for air while you sleep, don’t take it lightly. Your doctor can perform sleep tests on you to determine the severity of your condition.
In the meantime, don’t hesitate to make some changes to your bed or pillow to make you more comfortable if you have to change sleeping positions or elevate your neck. This is sometimes recommended as part of your treatment. Being comfortable can make the process a lot easier to adjust to. I would suggest a firm bed to keep you from sinking down and twisting your neck, further restricting your airway. You can also try a pillow specifically designed for head elevation and therapies such as the ones mentioned above.
If you know anybody who may be suffering from this condition or are curious as to whether or not they could have it, please feel free to share it because honestly, it could save their life and their relationship.